

Until the 20th century, two competing views of depression dominated clinical understanding: the psychoanalytic one, where one took a stand as “anger turned inward,” and the behavioural one, where it was viewed as a byproduct of environmental reinforcement, the only plausible explanation of the phenomenon as the result of “our environment.”
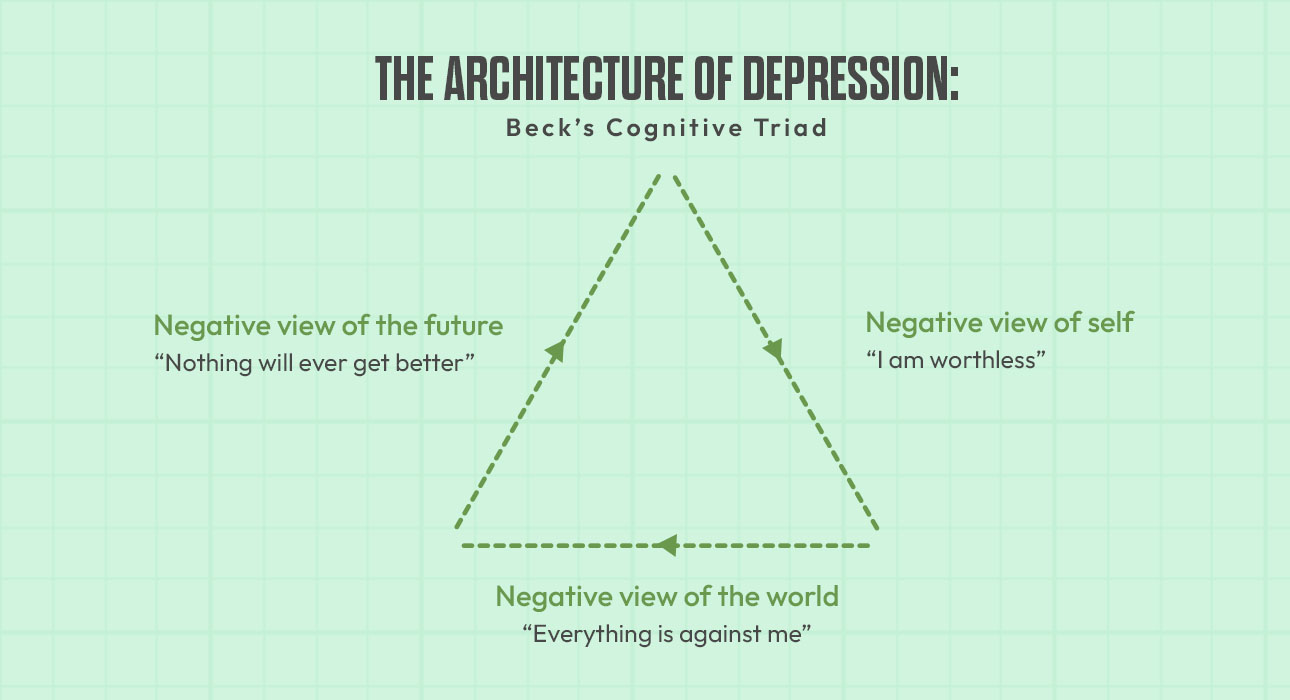
But in the 1960s, the landscape changed considerably with psychiatrist Aaron T. Beck’s pioneering efforts. By careful clinical observations, Beck discovered that the main disorder underlying depression was not emotional deficiency but a profound cognitive distortion (Beck, 1967). Beck’s fundamental notion, the Cognitive Triad, is the structural “architecture” of the depressive experience. He suggested that depression is perpetuated by a systematic bias in information processing, a triad of negative, automatic thoughts about the self, the world, and the future.
The Genesis of the Triad: A Theoretical Framework
As Beck states (1967), depression is not a mood disorder, but a cognitive disorder. The affective and physical symptoms of depression, such as feelings of lethargy, sleep disturbances, or persistent sadness, are symptoms of the way our minds are thinking and acting, he suggested. These negative thinking patterns that affect the mind of someone are referred to as the Cognitive Triad.
- Negative View of the Self: The person believes that he or she is bad, inadequate, or worthless. They assign negative experiences to a physical, mental, or moral defect in themselves.
- Negative View of the World: The individual sees out of place that the environmental context is making great demands (impossible to meet or insurmountable barriers). They see events in their life as just losses or deprivations.
- Negative View of the Future: The person thinks the ongoing hardship can never stop. When looking ahead, failure and suffering are an unending anticipation they look forward to, producing a sense of utter hopelessness.
These three elements, Beck added, drive negative feedback loops and therefore amplify each other. The individual who is stuck in this triad will shut out all positive experiences and exaggerate negative ones; this is known as cognitive distortion (Beck, Rush, Shaw, & Emery, 1979).
Quantitative Analysis and Factual Data
Decades of research have confirmed the validity of the Cognitive Triad. Longitudinal studies, as well as psychometrics, including those conducted in psychology, have shown results corroborating its role in depression for decades.
1. The Cognitive Triad Inventory (CTI)
Designed to measure the three components of Aaron T. Beck’s Cognitive Triad. For psychometric measures of depression, the three components are measured via the CTI. High scores on the Triad components are shown to be highly correlated in many studies with symptoms from the Beck Depression Inventory (BDI) (Pössel, 2009).
2. 30% Variance Factor
Negative cognitive styles, especially in the context of the “Future” (hopelessness), have been shown to account for up to 30–35% of the variance in depressive symptoms among students and young adults (Clark & Beck, 1999) in studies investigating the onset of depression.
3. Effectiveness of Intervention
Intervention studies suggest that treatment of major depressive disorder with Cognitive Behavioural Therapy (CBT) targeting the triad is effective at a rate of about 50–75% and often surpasses that of pharmacological treatments after long-term follow-up treatment (Hollon et al., 2006).
Deep Dive: The Structural Components
1. The Self as Defective
In the first arm of the triad, the poor attribute is that a person’s misfortune has been attributed to an inner shortfall. They feel unable to develop the qualities necessary for happiness, and therefore, they want something worthwhile. Example: Suppose a candidate doesn’t do well on one preliminary exam. Rather than attributing the failure to poor prep or to a complicated paper (external/unstable factors), they report, “I am intellectually incapable” (internal/stable factor).
2. The World as Overwhelming
The second arm is interpretive of ongoing experiences. They see their environments as a means of defeat. Even neutral occurrences are perceived as signs of world hatred or their own social isolation. For instance, if a peer does not respond on the first contact, the person thinks,” I am not able to understand the response of the person. People are inherently dismissive of me; the social world is a cold place where I don’t belong” (Beck, 2011).
3. The Future as Hopeless
The final arm is the most important for the perpetuation of chronic depression: hopelessness. This person no longer looks forward and observes only that their present suffering will continue to endure. For example, a student might think to himself, “No matter how hard I study for this upcoming cycle, the result will always be the same.” This belief results in “paralysis of the will.” This is similar to Seligman (1972) regarding the theory of learned helplessness, but Beck focuses on the cognitive assessment of that helplessness as the driving force.
The Triad’s Foundations: Cognitive Schemas
Triads exist in Schemas, which are internal, stable underlying beliefs developed in childhood and in early development. Beck (1967) defined schema as “cognitive structures that guide the screening, encoding, and retrieval of information.”
- Latent Schemas: A person may have a negative schema (such as a “I am incompetent” type of schema) that remains dormant until a specific life event elicits it.
- Information Processing Bias: Activated schemas are a filter. They lead the person to only focus on the information that backs up the negative attitude and ignore any “disconfirming evidence” (Kovacs & Beck, 1978).
How Does it Work: Cognitive Distortions
Between the underlying schemas and the automatic thoughts on either part of the Triad are Cognitive Distortions. These are logical misconceptions used by the brain to maintain the Triad:
- Arbitrary Inference: Drawing a conclusion when there is no evidence, or even when the evidence is contrary to the conclusion.
- Selective Abstraction: Focusing on a detail taken out of context while ignoring other, more salient features of the situation.
- Overgeneralization: Making a universal generalisation from one or more isolated instances and applying this concept in a bunch of unrelated contexts.
- Magnification and Minimisation: Evaluation errors that will give rise to either an increase in the importance of a negative event or a minor decrease in the importance of a positive event.
- Personalisation: Connection to some external event by relating it to oneself without justification.
Clinical Implications and CBT
CBT aims to assist the patient in identifying the Triad elements, resisting the elements of the Triad, and adapting the Triad.
- Behavioural Activation: Testing the “Future” arm, doing small actions when you need to show people that something could change.
- Cognitive Restructuring: Relying on “Socratic Questioning”: challenging the “Self” arm, for example: “What evidence do you have about your own failure?”
- Collaborative Empiricism: The therapist and patient work together as “co-investigators” to scientifically test the validity of the patient’s interpretations (Beck, 2011).
Theories Compared to Previous Cognitive Modelling
It is important to distinguish Beck’s model from others:
- Beck vs. Ellis: While Albert Ellis (REBT) centred around “Irrational Beliefs”, Beck centred around the process by which we think (distortions) and the content of the Triad (Beck, 1976).
- Beck vs. Seligman: Seligman’s Learned Helplessness emphasises the expectancy for non-contingency between actions and outcomes. Beck’s Triad builds on this idea, but it also considers “Self” and “World,” the two important drivers of the disorder, to be equally important (Seligman, 1972).
Conclusion
Beck’s Cognitive Triad is one of the main ideas in psychological theory because it makes a logical and empirical sense of depression. He claims that Beck’s model not only explains why people are prone to depressive symptoms but also contributes to improved cognitive control. By framing the disorder as a system of negative appraisals of the self, the world and the future, Beck steered the field closer to a more treatable conception of mental health.
Read More from Us
- Generalised Anxiety Disorder
- Dementia: Symptoms, Causes, Types, and Treatment
- How Stress Affects the Immune System: The Mind Body Connection
- Transpersonal Psychotherapy: Bridging Spirituality and Clinical Psychology
References +
- Beck, A. T. (1967). Depression: Causes and treatment. University of Pennsylvania Press. Beck, A. T. (1976). Cognitive therapy and the emotional disorders. International Universities Press.
- Beck, A. T., Rush, A. J., Shaw, B. F., & Emery, G. (1979). Cognitive therapy of depression. Guilford Press.
- Beck, J. S. (2011). Cognitive behaviour therapy: Basics and beyond (2nd ed.). Guilford Press.
- Clark, D. A., & Beck, A. T. (1999). Scientific foundations of cognitive theory and therapy of depression. Wiley.
- Hollon, S. D., Stewart, M. O., & Strunk, D. (2006). Enduring effects of cognitive therapy in the treatment of depression and anxiety. Annual Review of Psychology, 57, 285–315.
- Kovacs, M., & Beck, A. T. (1978). Maladaptive cognitive structures in depression. American Journal of Psychiatry, 135(5), 525–533.
- Pössel, P. (2009). Cognitive Triad Inventory (CTI): Psychometric properties and factor structure of the German translation. Journal of Behaviour Therapy and Experimental Psychiatry, 40(2), 240–247. Seligman, M. E. (1972). Learned helplessness. Annual Review of Medicine, 23, 407–412.